
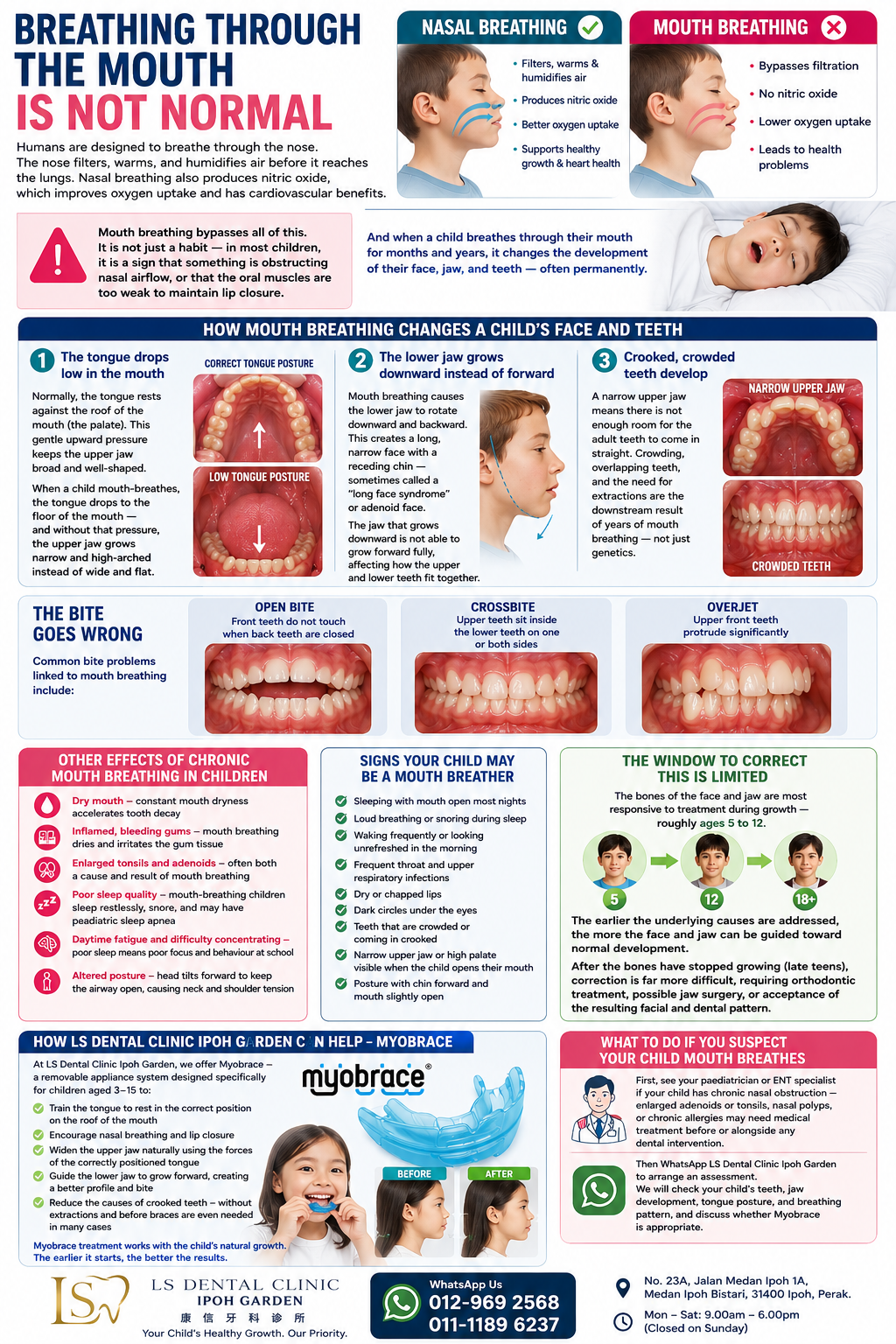
Breathing Through the Mouth Is Not Normal
Humans are designed to breathe through the nose. The nose filters, warms, and humidifies air before it reaches the lungs. Nasal breathing also produces nitric oxide, which improves oxygen uptake and has cardiovascular benefits.
Mouth breathing bypasses all of this. It is not just a habit — in most children, it is a sign that something is obstructing nasal airflow, or that the oral muscles are too weak to maintain lip closure.
And when a child breathes through their mouth for months and years, it changes the development of their face, jaw, and teeth — often permanently.
How Mouth Breathing Changes a Child's Face and Teeth
The bones of a child's face are soft and still growing. They are shaped by the forces applied to them — including the tongue, lips, cheeks, and airflow. When a child breathes through their mouth instead of their nose:
The tongue drops low in the mouth
Normally, the tongue rests against the roof of the mouth (the palate). This gentle upward pressure is what keeps the upper jaw broad and well-shaped. When a child mouth-breathes, the tongue drops to the floor of the mouth — and without that pressure, the upper jaw grows narrow and high-arched instead of wide and flat.
The lower jaw grows downward instead of forward
Mouth breathing causes the lower jaw to rotate downward and backward. This creates a long, narrow face with a receding chin — sometimes called a "long face syndrome" or adenoid face. The jaw that grows downward is not able to grow forward fully, affecting how the upper and lower teeth fit together.
Crooked, crowded teeth develop
A narrow upper jaw means there is not enough room for the adult teeth to come in straight. Crowding, overlapping teeth, and the need for extractions are the downstream result of years of mouth breathing — not just genetics.
The bite goes wrong
Common bite problems linked to mouth breathing include:
- Open bite — front teeth do not touch when the back teeth are closed
- Crossbite — upper teeth sit inside the lower teeth on one or both sides
- Overjet — upper front teeth protrude significantly
Other Effects of Chronic Mouth Breathing in Children
Beyond the face and teeth, mouth breathing causes:
- Dry mouth — constant mouth dryness accelerates tooth decay, especially in young permanent teeth
- Inflamed, bleeding gums — mouth breathing dries and irritates the gum tissue
- Enlarged tonsils and adenoids — often both a cause and result of mouth breathing
- Poor sleep quality — mouth-breathing children sleep restlessly, snore, and may have paediatric sleep apnea
- Daytime fatigue and difficulty concentrating — poor sleep means poor focus and behaviour at school
- Altered posture — the head tilts forward to keep the airway open, causing neck and shoulder tension
Signs Your Child May Be a Mouth Breather
Watch for:
- Sleeping with mouth open most nights
- Loud breathing or snoring during sleep
- Waking frequently or looking unrefreshed in the morning
- Frequent throat and upper respiratory infections
- Dry or chapped lips
- Dark circles under the eyes
- Teeth that are crowded or coming in crooked
- Narrow upper jaw or high palate visible when the child opens their mouth
- Posture with chin forward and mouth slightly open
The Window to Correct This Is Limited
The bones of the face and jaw are most responsive to treatment during growth — roughly ages 5 to 12. The earlier the underlying causes are addressed, the more the face and jaw can be guided toward normal development.
After the bones have stopped growing (late teens), soft tissue and skeletal correction is far more difficult, requiring orthodontic treatment, possible jaw surgery, or acceptance of the resulting facial and dental pattern.
How LS Dental Clinic Can Help — Myobrace
At LS Dental Clinic Ipoh Garden, we offer Myobrace — a removable appliance system designed specifically for children aged 3–15 to:
- Train the tongue to rest in the correct position on the roof of the mouth
- Encourage nasal breathing and lip closure
- Widen the upper jaw naturally using the forces of the correctly positioned tongue
- Guide the lower jaw to grow forward, creating a better profile and bite
- Reduce the causes of crooked teeth — without extractions and before braces are even needed in many cases
Myobrace treatment works with the child's natural growth. The earlier it starts, the better the results.
What to Do If You Suspect Your Child Mouth Breathes
First, see your paediatrician or ENT specialist if your child has chronic nasal obstruction — enlarged adenoids or tonsils, nasal polyps, or chronic allergies may need medical treatment before or alongside any dental intervention.
Then WhatsApp LS Dental Clinic Ipoh Garden to arrange an assessment. We will check your child's teeth, jaw development, tongue posture, and breathing pattern, and discuss whether Myobrace is appropriate.
The earlier you act, the more we can work with your child's growth — rather than trying to correct it after the fact.
Key Research References
- Luzzi V et al. (2021). Effects of mouth breathing on facial skeletal development in children: a systematic review and meta-analysis. European Journal of Paediatric Dentistry. PMC Full Text
- Karan A et al. (2022). The impact of mouth breathing on dentofacial development: A concise review. Journal of Indian Orthodontic Society. PMC Full Text
- Verma R et al. (2025). Early Intervention for Malocclusion: Role of Myobrace in Children Aged 6–10 Years. PMC. PMC Full Text — 70% shift to nasal breathing, 80% improved tongue posture with Myobrace
